Subtle manifestations of cGVHD can go undiagnosed for months—so actively monitor all patients1‐3
- Evaluate all new symptoms after transplant as potential signs of cGVHD4
- Educate patients and caregivers to recognize the early signs of cGVHD and report any changes to their posttransplant care team
- Use contextual questions to help patients recognize and express their symptoms
According to NIH cGVHD Diagnosis and Staging Consensus recommendations, early intervention may5
- Prevent progression to severe cGVHD
- Relieve symptoms


As a physician, I must rely on my patients to track changes in their recovery journey and share them with me.
Corey S. Cutler, MD, MPH
GVHD Expert
Helpful approaches to ensure early identification of cGVHD
The following resources can support conversations with your patients and their caregivers.
Patient education: Day 100 Post Transplant Master Class Video Series
This video series, developed in partnership with the American Society for Transplantation and Cellular Therapy (ASTCT), features cGVHD experts who provide step-by-step instruction on how patients can play a critical role in their self-care from day 100 and beyond.
Explore the Day 100 Series

Prezerve™ post-transplant symptom tracker app
An ideal resource to provide upon discharge, the Prezerve™ app helps patients and their caregivers detect early symptoms of cGVHD and connect to support via care center site ID.
Learn about the trackerA patient counseling resource for you and your patients
The Early Identification of Symptoms Associated With Chronic Graft-Versus-Host Disease Brochure supports a discussion of the importance of patient education and proactive symptom monitoring.
Download the brochureOrgan scoring to assess disease severity5
Signs and symptoms of cGVHD vary among patients and over time. This assessment features NIH cGVHD Diagnosis and Staging Consensus recommendations for scoring organs on a 0 to 3 scale, from no involvement/no symptoms to severe functional compromise.

Swipe to view the
whole chart
| Score 0 | Score 1 | Score 2 | Score 3 | |
|---|---|---|---|---|
Performance score: ___ ECOG KPS LPS | Asymptomatic and fully active (ECOG, 0; KPS or LPS, 100%) | Symptomatic, fully ambulatory, restricted only in physically strenuous activity (ECOG, 1; KPS or LPS, 80%-90%) | Symptomatic, ambulatory, capable of self-care, >50% of waking hours out of bed (ECOG, 2; KPS or LPS, 60%-70%) | Symptomatic, limited self-care, >50% of waking hours in bed (ECOG, 3-4; KPS or LPS, <60%) |
Skin features | No sclerotic features | Superficial sclerotic features | Deep sclerotic features, impaired mobility, ulceration | |
Skin GVHD scored by BSAa:Maculopapular rash/erythema, lichen planus–like features, sclerotic features, papulosquamous lesions or ichthyosis, keratosis pilaris–like GVHD | No BSA involved | 1%-18% BSA | 19%-50% BSA | >50% BSA |
Skin GVHD not scored by BSA:Hyperpigmentation, hypopigmentation, poikiloderma, severe or generalized pruritus, hair involvement, nail involvement | ||||
Mouth:Lichen planus–like features | No symptoms | Mild symptoms with disease signs but not limiting oral intake significantly | Moderate symptoms with disease signs with partial limitation of oral intake | Severe symptoms with disease signs on examination with major limitation of oral intake |
Eyes:KCS confirmed by ophthalmologist | No symptoms | Mild dry eye symptoms not affecting ADL | Moderate dry eye symptoms partially affecting ADL | Severe dry eye symptoms significantly affecting ADL or unable to work because of ocular symptoms or loss of vision due to KCS |
GI tract:Esophageal web/proximal stricture, dysphagia, anorexia, nausea, vomiting, diarrhea, weight loss,b failure to thrive | No symptoms | Symptoms without significant weight lossb (<5%) | Symptoms associated with mild to moderate weight lossb (5%-15%) or moderate diarrhea without significant interference with daily living | Symptoms associated with significant weight lossb (>15%), requires nutritional supplement or esophageal dilation for most calorie needs, or severe diarrhea with significant interference with daily living |
Liver | Normal total bilirubin and ALT or ALP <3 × ULN | Normal total bilirubin with ALT ≥3 to 5 × ULN or ALP ≥3 × ULN | Elevated total bilirubin but ≤3 mg/dL or ALT >5 × ULN | Elevated total bilirubin >3 mg/dL |
Lungsc | No symptoms | Mild symptoms (shortness of breath after climbing 1 flight of steps) | Moderate symptoms (shortness of breath after walking on flat ground) | Severe symptoms (shortness of breath at rest; requiring O2) |
Lung score: % FEV1 | FEV1 ≥80% | FEV1 60%-79% | FEV1 40%-59% | FEV1 ≤39% |
Genital tract:Currently sexually active (yes/no) | No signs | Mild signs; females with or without discomfort on examination | Moderate signs and may have symptoms with discomfort on examination | Severe signs with or without symptoms |
Joints and fascia:P-ROM score Shoulders (1-7): ____ Elbows (1-7): ____ Wrists/fingers (1-7): ____ Ankles (1-4): ____ | No symptoms | Mild tightness of arms or legs, normal or mild decrease in range of motion and not affecting ADL | Tightness of arms or legs or joint contractures, erythema thought to be due to fasciitis, moderate decrease in range of motion, and mild to moderate limitation of ADL | Contractures with significant decrease in range of motion and significant limitation of ADL (unable to tie shoes, button shirt, dress self, etc) |
Other indicators, clinical features, or complications related to cGVHD:Ascites (serositis), eosinophilia >500/μL, myasthenia gravis, nephrotic syndrome, pericardial effusion, peripheral neuropathy, platelet count <100,000/μL, pleural effusion, polymyositis, weight loss >5% without gastrointestinal symptoms | ||||
aSkin scoring should use both percentage of BSA involved by disease signs and the cutaneous features scales. When a discrepancy exists between the percentage of BSA score and the skin feature score, or if superficial sclerotic features are present but there is impaired mobility or ulceration, the higher level should be used for the final skin scoring.
bWeight loss within 3 months.
cLung scoring should be performed using both the symptoms and FEV1 scores whenever possible. FEV1 should be used in the final lung scoring when there is a discrepancy between symptoms and FEV1 scores.
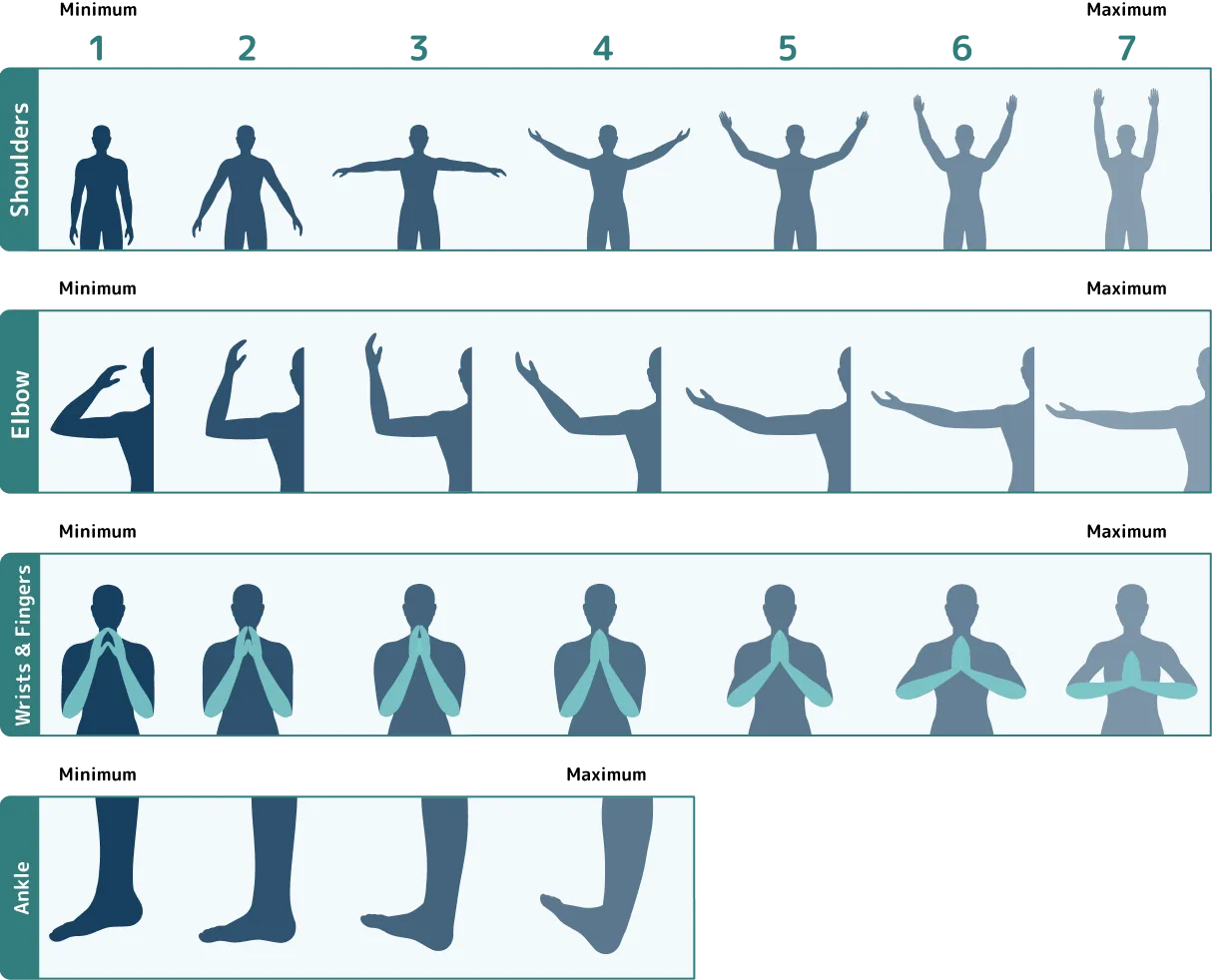
Range of motion to assess joints and fascia6
The Photographic Range of Motion (P-ROM) scale is an important tool for assessing joint and fascial GVHD. It assesses the active range of motion of multiple joints, grades the severity of involvement, and helps monitor response to treatment. The P-ROM scale features a series of images that depict a range of motion for shoulders, elbows, wrists/fingers, and ankles. The P-ROM total score is the sum of scores in all 4 joints, with a maximum possible score of 25.
Swipe to view the
whole chart
Flexibility6
ADL=activities of daily living; ALP=alkaline phosphatase; ALT=alanine transaminase; BSA=body surface area; cGVHD=chronic graft-versus-host disease; ECOG=Eastern Cooperative Oncology Group; FEV1=forced expiratory volume in first second of expiration; GI=gastrointestinal; KCS=keratoconjunctivitis sicca; KPS=Karnofsky Performance Status; LPS=Lansky Performance Status; NIH=National Institutes of Health; ULN=upper limit of normal.
References: 1. Hildebrandt GC, Fazekas T, Lawitschka A, et al. Diagnosis and treatment of pulmonary chronic GVHD: report from the consensus conference on clinical practice in chronic GVHD. Bone Marrow Transplant. 2011;46(10):1283-1295. 2. Nassiri N, Eslani M, Panahi N, Mehravaran S, Ziaei A, Djalilian AR. Ocular graft versus host disease following allogeneic stem cell transplantation: a review of current knowledge and recommendations. J Ophthalmic Vis Res. 2013;8(4):351-358. 3. Lee SJ, Vogelsang G, Flowers MED. Chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2003;9(4):215-233. 4. Lee SJ, Flowers MED. Recognizing and managing chronic graft-versus-host disease. Hematology Am Soc Hematol Educ Program. 2008;228(1):134-141. 5. Jagasia MH, Greinix HT, Arora M, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol Blood Marrow Transplant. 2015;21(3):389-401.e1. 6. Hidalgo Calleja C, Martín Hidalgo D, Román Curto C, et al. Graft versus host disease-related eosinophilic fasciitis: cohort description and literature review. Adv Rheumatol. 2022;62(1):33. doi:10.1186/s42358-022-00262-3.